Article View
Strabismus
Sagging Eye Syndrome (SES)
Orthoptics in surgical strubismus
Cyclophoria
Inferior Oblique Muscle
Superior Oblique Muscle
Lateral Rectus
Medial Rectus
Inferior Rectus management in orthoptics
Superior Rectus
Pediatric Strabismus Management in Orthoptics
Adult strabismus management
Comorbidities and Complications in Strabismus Management: An Orthoptic Perspective
Choose your reading experience
Strabismus
Sagging Eye Syndrome (SES)
Abstract
Sagging Eye Syndrome (SES) represents one of the most significant oculomotor disorders affecting the elderly population. The term "sag" refers to the drooping or sagging of the eye due to the relaxation and eventual rupture of soft tissues within Tenon's membrane that connect the superior rectus and lateral rectus muscles. This age-related condition has gained increased recognition in recent years due to advances in imaging technology and our understanding of orbital anatomy.
Historical Background
Early Recognition: ARDET (2009)
The journey to understanding SES began in 2009 with the description of ARDET (Age-Related Distance EsoTropia). This condition was characterized as an acquired form of strabismus affecting elderly patients, presenting with:
Greater esotropia at distance fixation without abnormal ductions or versions
Balanced fusion amplitudes or slight divergence insufficiency
Orthophoria at near vision
The Breakthrough: Joseph L. Demer's Research (2013)
The syndrome was formally described in 2013 by the team of Joseph L. Demer, thanks to advances in MRI technology and the study of pulley system evolution.
Anatomy and Pathophysiology
Normal Orbital Anatomy
The eye is covered by Tenon's capsule, a thin fibro-elastic membrane that:
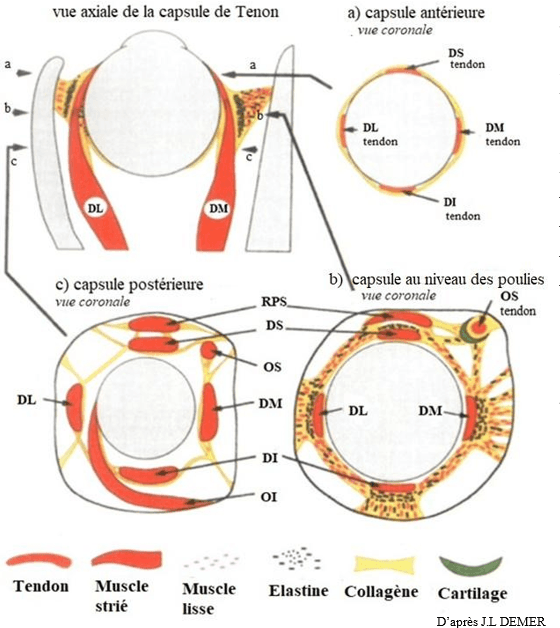
Begins at the limbal sclera
Surrounds the eyeball and optic nerve
Forms a cavity in which the globe moves
Separates the eye from orbital fat
Extends muscle sheaths onto the scleral surface
At the posterior pole of the eye, connective tissue bands called "pulleys" (from the Greek word for "pivot") connect to the rectus muscles and are located anterior to the orbital wall. These pulley bands serve crucial functions:
Stabilizing muscle trajectories
Playing an important role in ocular movements
Determining the force directions of extraocular muscles
Pathological Changes in SES
MRI studies have revealed the progressive changes that occur in SES:
Early Stage (ARDET): Marked elongation of the LR-SR band (lateral rectus-superior rectus band) with sagging of the lateral rectus muscle

Advanced Stage (SES): Complete rupture of the LR-SR band with significant displacement of the lateral rectus muscle downward and inward
Associated Changes:
Elongation and curvature of superior and inferior rectus muscles
Aponeurotic ptosis with levator muscle detachment
Optic nerve coiling
Superior palpebral sulcus defects
MRI Findings
Advanced imaging techniques allow visualization of:

The LR-SR band integrity
Muscle displacement patterns
Angle measurements showing displacement (normal vs. >101° in SES)
Bilateral involvement patterns
Clinical Characteristics
Primary Signs
SES presents with distinctive clinical features that vary depending on whether the condition is unilateral or bilateral:
Asymmetric Involvement:
Minimal distance esotropia
Hypotropia and excyclotorsion of the affected eye
Symmetric Involvement:
Minimal distance esotropia without vertical component
Associated Oculo-Palpebral Changes
Due to the aging process, SES often presents alongside:
Ptosis (drooping eyelids)
Dermatochalasis (excess eyelid skin)
Lipoptosis (fat pad prolapse)
Superior tarsal sulcus hollowing
Triggering Factors
SES symptoms often become apparent after ocular surgeries that improve vision:
Cataract surgery: Previously, cataracts may mask visual disturbance and diplopia. Once removed, diplopia becomes evident, sometimes leading to wrongful blame of the surgeon or anesthesia
Cosmetic eyelid procedures: Dermatochalasis correction, lipoptosis surgery
Botulinum toxin injections
Clinical Examination and Orthoptic Assessment
Functional Symptoms
Poorly defined visual disturbance at distance
Distance diplopia
Generally asymptomatic at near vision
Motility Assessment
Versions: Minimal limitation of abduction in one or both eyes, or essentially normal
Ductions: Generally balanced
Deviation Measurements
Distance: Esotropia
Near: Orthophoria to esophoria
No torticollis or abnormal head posture
No version incomitance or fixation-dependent incomitance
Binocular Vision Studies
Comprehensive assessment includes:
Stereotests
Worth 4-dot test
Vergence testing
Synoptophore examination for correspondence
Diplopia Analysis
Homonymous diplopia at distance (symmetric involvement)
Associated vertical diplopia (hypotropia) and excyclotorsion in the more affected eye (asymmetric involvement)
Coordimetry
Confirms deviation patterns on diagrams, providing valuable evolutionary and medical documentation.
Case Studies
Case 1: Mrs. Monique B. (80 years old)

Presentation: Homonymous diplopia in all gaze directions since late 2010
History: Bilateral cataract surgery late 2016-early 2017
Referral: May 2017 for worsened diplopia
Treatment: 30Δ base-out prism trial, surgical intervention planned
Outcome: Demonstrates typical post-cataract surgery revelation of SES
Case 2: Mrs. D.F. (82 years old)
History: Bilateral cataract surgery September-October 2016
Progressive management: Escalating prism correction from 6Δ to 8Δ base-out
Findings: 3° excyclotorsion left eye, second-degree binocular vision
Management: Combined incorporated and press-on prisms
Treatment Options
Non-Surgical Management
Prism Correction:
Press-on prisms for trial periods
Incorporated prisms in spectacle lenses
Progressive increase often necessary
Monitoring:
Regular orthoptic surveillance
Documentation of progression
Generally progressive condition
No Role for Orthoptic Exercises:
Traditional orthoptic rehabilitation is not effective
Mechanical nature of the problem prevents muscle training success
Surgical Management
When prism correction becomes inadequate:
Bilateral Medial Rectus Recession:
Indicated for symmetric cases
Addresses the convergent strabismus
Kaufmann and Krzizok Technique:
Lateral rectus elevation procedure
Addresses the mechanical displacement
Restores more normal muscle geometry
Differential Diagnosis
ARDET (Age-Related Distance EsoTropia)
Very similar to SES
Represents earlier stage with band elongation but no rupture
Minimal distance esotropia related to Tenon's capsule aging
Muscle displacement without LR-SR band rupture
Divergence Paralysis/Insufficiency
Key distinguishing features:
Always associated with neurological causes:
Intracranial hypertension or hypotension
Brain tumors
Head trauma
Multiple sclerosis
Chiari malformation
Miller-Fisher syndrome
Spinocerebellar ataxia type 3 (Machado-Joseph disease)
MRI is essential for evaluation
Sixth Nerve Palsy
Distinguishing incomitances:
Esotropia greater than esophoria (distance/near difference)
Fixation-dependent variation
Gaze-dependent variation
Secondary deviation greater than primary (Hering's and Sherrington's laws)
Decompensated Esophoria/Esotropia
Comitant deviation at distance and near
Large angle deviation
Progressive increase over time
Esophoria decompensates into tropia
Heavy Eye Syndrome (HES) and High Myopia
Characteristics:
Significant myopic anisometropia
Convergent vertical strabismus
More myopic eye typically lower
May progress to strabismus fixus
Related to eyeball shape changes in high myopia
Nasal displacement of superior and inferior rectus muscles
Downward displacement of lateral rectus muscle
Thyroid Eye Disease (Orbitopathy)
Distinguishing features:
Affects all orbital structures
Inflammatory signs: pain on eye movement, chemosis, conjunctival redness
Functional symptoms: tearing, photophobia, asthenopia, retro-orbital pain
Various diplopia patterns
Eyelid retraction (upper > lower)
Exophthalmos
True myopathy with restrictive pattern
Myasthenia Gravis
Key characteristics:
Autoimmune neuromuscular junction disorder
Variable deviation patterns
Variable ptosis
Fatigability with sustained effort
Poor nerve-to-muscle transmission
Symptoms worsen with fatigue
Conclusion
Sagging Eye Syndrome represents a significant age-related oculomotor disorder that requires:
Key Points for Clinicians:
Non-neurological origin: Unlike many adult-onset strabismus conditions, SES is mechanical, not neurological
Progressive nature: The condition typically worsens over time, requiring ongoing management
Post-surgical revelation: Often becomes symptomatic after vision-improving procedures
Imaging importance: MRI provides crucial diagnostic information about band integrity and muscle displacement
Treatment challenges: Requires combination of optical and potentially surgical management
Clinical Significance:
Affects elderly population with increasing prevalence
Can be unilateral or bilateral, symmetric or asymmetric
Causes distance esotropia with near orthophoria initially
May progress to include vertical and torsional components
Requires differentiation from neurological causes of diplopia
Management Approach:
Orthoptic monitoring is essential
Prism correction often provides initial relief
Surgical intervention may become necessary
Patient education about progressive nature is important
The recognition and understanding of SES has significantly improved with advances in orbital imaging and the pioneering work of researchers like Joseph L. Demer. As our population ages, familiarity with this condition becomes increasingly important for ophthalmologists, orthoptists, and other eye care professionals.
Remember: SES ≠ ARDET - While related, these represent different stages of the same pathological processo, with SES being the more advanced form involving complete band rupture rather than just elongation.
© VisReed 2025
By two creative minds